Nghp Po Box 138832 Oklahoma City Ok 73113
NGHP PO Box 138832 Oklahoma City OK 73113 Fax. Box 138856 Oklahoma City OK 73113.
Ok Franco Signor Final Settlement Detail Document Fill And Sign Printable Template Online Us Legal Forms
To ask questions regarding MSP recovery demand letters.

. Box 138868 Oklahoma City OK 73113. Oklahoma City OK 73113 Self-Calculated Conditional Payment Amount Option and fixed Percentage Option. All NGHP checks and inquires including Liability No-Fault Workers Compensation Congressional FOIA Bankruptcy Liquidation Notices and QICALJMSPRC NGHP PO.
NGHP PO Box 138832 Oklahoma City OK 73113 Fax. Oklahoma City OK 73113 Special Projects. NGHP PO Box 138832 Oklahoma City OK 73113 Fax.
All Product Liability Case Inquiries and Special Project Checks Special Projects. Every year on the anniversary of your settlement date you need to fill out the annual attestation form and submit it via Medicaregov or mail it to the Benefits Coordination Recovery Center. Enter a numeric value decimals and commas are optional.
CONSENT TO RELEASE The language below should be used when you a Medicare beneficiary want to authorize someone other than your attorney or other representative to receive information including identifiable health information from the. Commercial Repayment Center - NGHP PO Box 269003 Oklahoma City OK 73126. Oklahoma City OK 73113.
PO Box 138832. Non-Group Health Plan NGHP Inquiries and Checks. Total Amount of the Settlement Attorney Fee Amount Additional Procurement Expenses Please submit an itemized listing of these expenses Date the Case Was Settled Settlement Information Provided By Date The completed form should be sent to Medicare Secondary Payer Recovery Contractor NGHP PO Box 138832 Oklahoma City OK 73113 If you have any.
Please retain a COPY of this cover sheet for any future correspondence. For Recovery Agent Authorizations on CRC cases write to. GHP and Non Group Health Plans NGHP submit coverage.
To obtain Medicares final recovery claim amount. NGHP PO Box 138832 Oklahoma City OK 73113 Fax. To ask questions with respect to a Notice of Intent to Refer Debt to the.
All Product Liability Case Inquiries and Special Project Checks MSPRC Special Projects PO. Oklahoma City OK 73113. Commercial Repayment Center - NGHP PO Box 269003 Oklahoma City OK 73126 Phone.
Oklahoma City OK 73113. Amount Additional Procurement Expenses Please submit an itemized listing of these expenses Date the Case Was Settled Settlement Information Provided By Date The completed form should be sent to Medicare Secondary Payer Recovery Contractor NGHP PO Box 138832 Oklahoma City OK 73113 If you have any questions concerning this matter please call the Medicare. Please make several copies of this form because you must send this form to the Medicare contractor each year until all of your WCMSA has been spent.
To obtain conditional payment amounts. NGHP PO Box 138832. Box 138832 Oklahoma City OK 73113.
If cents are not entered the MSPRP will store the amount with zero cents. 405 869-3309 Data Entry Requirements. CONSENT TO RELEASE The language below should be used when you a Medicare beneficiary want to authorize someone other than your attorney or other representative to receive information including identifiable health information from the.
For BCRC cases when you select the Request a mailed copy of the conditional payment letter action the MSPRP will send the conditional payment letter to each authorized individualentity associated to the case ie the beneficiary and each individualentity. 2014 Dec Dallas CMS Revised Paperpdf Dallas Bar Association. Non-Group Health Plan NGHP Inquiries and Checks eg.
Dec 12 2013. Box 138832 Oklahoma City OK 73113. This form should be completed annually and mailed to NGHP PO BOX 138832 OKLAHOMA CITY OK 73113.
Contact the BCRC regarding any of the following. PO Box 138832. You can enter cents as well.
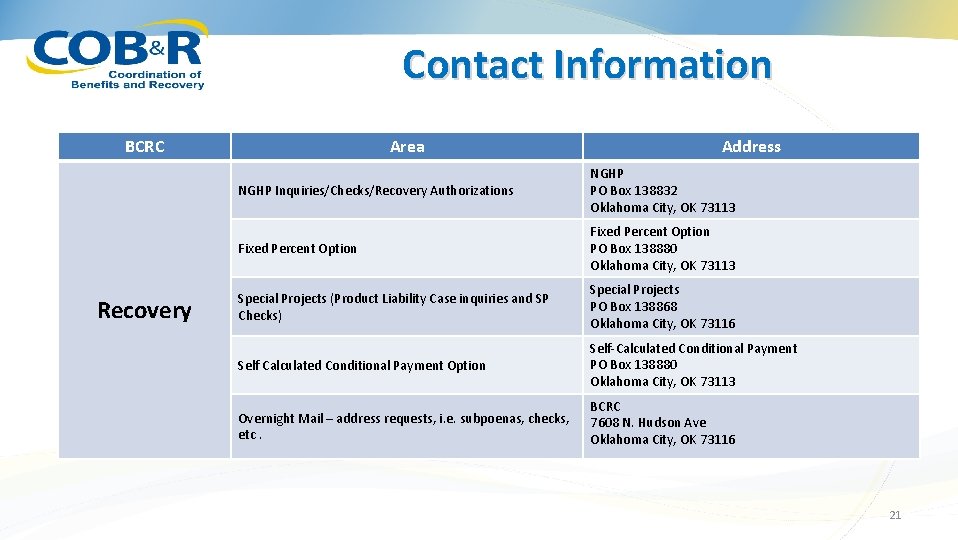
The information above will ensure accuracy when handling your case documentation Please indicate the type of. 10012016 unless fixed by Congress. NGHP PO Box 138832 Oklahoma City OK 73113 Fixed Percent Option Fixed Percent Option PO Box 138880 Oklahoma City OK 73113 Special Projects Product Liability Case inquiries and SP Checks Special Projects PO Box 138868 Oklahoma City OK 73116 Self Calculated Conditional Payment Option.
855 798-2627 For CRC cases write to. This will start one year from the date of settlement. 03012016 Last Modified.
Medicare Will Send Out a Conditional Payment Letter. BCRC NGHP PO Box 138832 Oklahoma City OK 73113. NGHP Correspondence Cover Sheet Keywords NGHP Correspondence Created Date.
NGHP PO Box 138832 Oklahoma City OK 73113 Fixed Percent Option Fixed Percent Option PO Box 138880 Oklahoma City OK 73113 Special Projects Product Liability Case inquiries and SP Checks Special Projects PO Box 138868 Oklahoma City OK 73116 Self Calculated Conditional Payment Option. For example a settlement amount of 10000. Please make several copies of this form because you must send this form to the Medicare contractor each year until all of your WCMSA has been spent.
Oklahoma City OK 73113-8832. MSPRC NGHP PO Box 138832 Oklahoma City OK 73113 By Fax 405 829-3309. Special Project Inquiries eg.
NGHP Correspondence Cover Sheet April 2018 Author. MSPRC NGHP PO. Oklahoma City OK 73113.
Please make several copies of this form because you must send this form to the Medicare contractor each year until all of your WCMSA has been spent. Send Medicare Final Settlement Details. Remember Medicare calls this money conditional payments Example of a Conditional Payment Letter 5.
Oklahoma City OK 73113-8897. This form should be completed annually and mailed to NGHP PO BOX 138832 OKLAHOMA CITY OK 73113 starting one year from the date of settlement. Submit correspondence to the BCRC address listed below Liability Insurance No-Fault Insurance Workers Compensation NGHP PO Box 138832 Oklahoma City OK 73113.
Where to Submit a Consent to Release document MSPRC - NGHP PO Box 138832 Oklahoma City OK 73113 Fax 405 869-3309 MODEL LANGUAGE CONSENT TO RELEASE The language below should be used when you a Medicare beneficiary want to. This letter should say how money Medicare has paid. MSPRC Correspondence On your fax coversheet please identify your correspondence as GHP or NGHP 405-869-3309.
This form should be completed annually and mailed to NGHP PO BOX 138832 OKLAHOMA CITY OK 73113 starting one year from the date of the settlement.
Benefits Coordination And Recovery Center Bcrc Overview Agenda

Free Medicare Consent To Release Form Medical Records Pdf Eforms
Cms Correspondence Cover Sheet Fill Online Printable Fillable Blank Pdffiller



Comments
Post a Comment